Chemotherapy and radiation remain central to modern cancer treatment, yet they often place a heavy burden on the body, affecting everything from your ability to eat and speak to the health of your skin and nerves. For patients and clinicians alike, addressing these treatment-related complications continues to be a persistent challenge. In response, oncologists have begun exploring light-based approaches as a way to reduce these secondary burdens.
Light has shaped life on Earth since the first single-celled organisms used it to generate energy billions of years ago — and your cells still respond to specific wavelengths in ways that influence not just sleep-wake cycles but also healing. Photobiomodulation (PBM) is a treatment approach that harnesses this relationship between light and biology, with research backing its benefits in various medical fields.
Europe has recently taken a significant step in bringing this therapy into mainstream cancer care. A newly released guide represents the first comprehensive European standard for using PBM in oncology, establishing standards for a therapy that many clinicians have yet to fully explore.1 This development reflects a broader shift in how supportive cancer care is being approached.
Europe Sets a Formal Framework for PBM in Oncology
In October 2025, the French-speaking Association for Supportive Care in Cancer (AFSOS) introduced the first European reference guide for the use of PBM in oncology. The announcement was made during the 16th National Congress of Oncology Supportive Care, held in Lille, France. This marks the first formal clinical standard for PBM in European oncology.2
• The guide sets clear clinical standards for PBM use — Led by Dr. Antoine Lemaire of Valenciennes General Hospital, the guide outlines when and how PBM should be integrated into supportive cancer care. It emphasizes that many clinicians remain unfamiliar with PBM despite its growing evidence base, and it positions the new reference document as a tool to close this knowledge gap. The aim is to standardize usage, so patients receive consistent care across treatment centers.
• Well-established uses of PBM across supportive cancer care — Cancer treatments place significant stress on tissues that divide rapidly or rely on delicate structural integrity, such as the lining of the mouth, skin, nerves, and connective tissue. Among PBM’s applications in oncology, the strongest clinical support exists for treating mucositis and radiodermatitis, both of which are common and painful complications of cancer treatment.
Mucositis refers to the painful inflammation and ulceration of the mucous membranes lining the digestive tract, which can make eating and swallowing extremely difficult for patients undergoing chemotherapy or radiation. Radiodermatitis refers to skin damage caused by radiation exposure and can range from redness and dryness to blistering and open wounds. It is common in breast, head and neck, and pelvic cancers.3
• The guide also covers other applications where evidence is moderate but promising — These conditions span multiple types of tissue and treatment-related complications, including:4,5
◦Lymphoedema — Persistent swelling caused by impaired lymphatic drainage after surgery or radiation.
◦Xerostomia — Dry mouth resulting from salivary gland damage during head and neck radiation treatment.
◦Trismus — Restricted jaw movement linked to muscle or joint stiffness after radiation.
◦Osteoradionecrosis — Bone injury and breakdown caused by impaired blood flow after radiation.
◦Dysphagia — Difficulty swallowing due to tissue inflammation or neuromuscular impairment.
◦Dysphonia — Voice changes or hoarseness from irritation or injury to vocal structures.
◦Dysgeusia — Altered or reduced taste perception related to chemotherapy.
◦Chemotherapy-induced neuropathy and alopecia — Nerve pain, numbness, and hair loss triggered by cytotoxic drugs.
◦Palmoplantar erythroderma — Redness, swelling, and tenderness of the palms and soles linked to certain chemotherapies.
• PBM delivers low-intensity light to stimulate mitochondrial activity without heat — The guide describes PBM therapy as “a mechanism in which red, near infrared, or blue light is delivered to damaged target tissues.” The approach relies on controlled light exposure rather than thermal effects and is applied using devices selected according to tissue depth and treatment location.
However, while the guide includes blue light within its technical definition of PBM, I do not recommend artificial blue light exposure for therapeutic use, as it disrupts circadian signaling and has well-documented effects on sleep regulation, hormonal balance, and systemic health. For this reason, red and near-infrared wavelengths remain the focus of safer and more biologically aligned applications.
• Around 100 cancer centers in France are currently equipped with PBM devices — These clinics use either laser or light-emitting diode (LEDs) equipment. While lasers tend to deliver more focused penetration, LEDs provide broader diffusion, and both can be effective depending on the clinical need. The choice of tool, treatment duration, and dosing parameters all depend on the area being treated and the depth of tissue involvement.
Therapeutic dosing generally falls within the range of 10 to 12 joules per square centimeter, but each device has its own set of instructions to ensure the light reaches the target tissue at the correct strength. Sessions typically last about 20 minutes, often administered once or twice per week in protocols that span eight to 16 sessions. Adjustments are made based on symptom severity and location.
• The therapy is also expanding beyond oncology — Private clinicians increasingly use these devices in sports medicine and gynecologic care, while patient associations advocate for broader access. Some patients now request PBM directly, which raises the need for oncology clinicians to understand PBM and recognize appropriate indications within cancer care pathways.
• Despite growing adoption in clinical settings, PBM faces several barriers to wider use — The most pressing is the lack of dedicated reimbursement. At present, the cost of PBM is typically bundled into consultation fees, which limits its scalability.
The guide raises concerns about the rise of home-use PBM devices, noting that many sold online lack proper safety certification, deliver inadequate or poorly calibrated doses, or emit wavelengths that can pose health risks. While this caution is valid, it’s also important to recognize that not all consumer devices fall into this category.
When properly designed, dosed, and used with informed guidance, some at-home units can be a useful part of a broader therapeutic approach. The key is understanding how to choose equipment that’s both safe and effective. I’ll go into more detail later on how to evaluate devices and what to look for if you’re considering one for personal use.
By laying out clear protocols, validated use cases, and technical considerations, the new European guide brings much-needed structure to a therapy that has, until now, been applied unevenly across clinics. To understand why European oncologists are standardizing PBM protocols, it helps to grasp how light actually interacts with your cells.
Understanding the Science Behind Light
Not all light affects your body the same way. What matters is the wavelength — essentially, how long or short each wave of light is, measured in nanometers. Each part of the light spectrum interacts with your cells differently, and only a specific range carries the ability to penetrate deeply enough to influence healing, energy production, and inflammation without causing harm.
• Solar rays can be divided into three categories — Ultraviolet (UVA, UVB, and UVC) account for 7% of the solar spectrum. Visible light (violet, indigo, blue, green, yellow, orange, red), ranging from 400 to 700 nanometers, accounts for 39% of the spectrum. Invisible infrared (near-, mid-, and far-infrared) light, ranging from 700 to 10,000 nanometers, accounts for 54% of the spectrum.
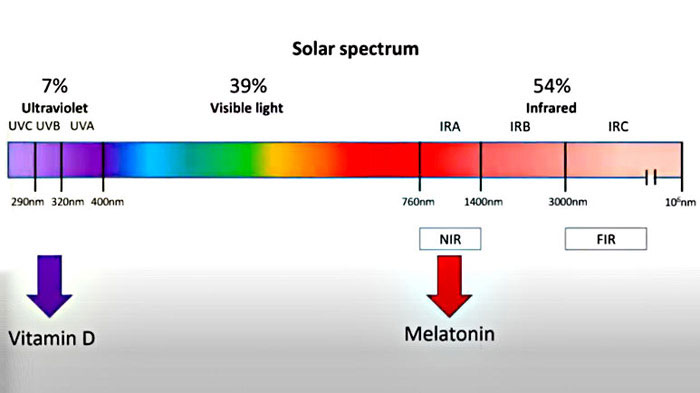
• This range is called the optical window — The ideal optical window is about halfway through the near-infrared range, between 600 and 900 nanometers. Within this optical window, the wavelengths are long enough to penetrate the body and reach deep into the tissues, but they’re not readily absorbed by hemoglobin, melanin, and water. The optical window sweet spot is around 800 to 810 nanometers.
• Penetration depth varies by wavelength — Red light starts around 600 nanometers. In the range of about 630 to 660 nanometers, red light typically reaches a few millimeters into tissue, making it relevant for skin and superficial structures. Meanwhile, near-infrared light begins above 700 nanometers. At around 800 to 850 nanometers, it penetrates much deeper, reaching muscles, joints, and other underlying tissues.
Longer wavelengths, closer to 1,050 nanometers, can penetrate even further, with research exploring their interaction with deeper tissue and neural structures, although these applications remain an active area of investigation.
• The key target within your cells is an enzyme called cytochrome c oxidase — This is a protein embedded in your mitochondria that acts as the final gatekeeper in cellular energy production. When this enzyme absorbs red or near-infrared light, it accelerates the production of adenosine triphosphate (ATP), the molecule your body uses for cellular energy. This increase in ATP supports everything from tissue repair to immune signaling and metabolic resilience.
• PBM influences melatonin production, but not the kind produced by your brain at night — Instead, near-infrared light stimulates melatonin synthesis inside the mitochondria, which account for roughly 95% of the melatonin produced in your body. By comparison, the melatonin secreted by the pineal gland during nighttime represents only 5% of your body’s total melatonin output.
Within mitochondria, melatonin serves as a powerful antioxidant. It neutralizes free radicals generated during normal energy production and helps protect mitochondrial structures from oxidative damage. Because mitochondria are present in nearly every cell, this mechanism helps explain why red and near-infrared light can exert effects across such a wide range of tissues.
• Nitric oxide is another key player — When light triggers its release from cellular storage sites, it leads to improved circulation by widening blood vessels and reducing inflammation. The result is better blood flow to damaged tissues, improved oxygen delivery, and support for immune and repair processes in areas under stress.
This broad impact on core biological functions has made PBM an area of growing interest in fields beyond oncology. To get a deeper look at how different wavelengths work in the body and what makes them therapeutically active, read “Exploring Benefits of Different Wavelengths of Light in Photobiomodulation.”
Other Health Benefits of PBM Beyond Cancer Care
A clinical consensus published in the Journal of the American Academy of Dermatology reviewed the available evidence on PBM and found that it shows therapeutic benefit for the following conditions:6
• Wound healing — Chronic wounds can persist for weeks or months due to poor blood flow, infection risk, or high levels of inflammation. This includes diabetic foot ulcers, venous leg ulcers, pressure ulcers (bedsores), and burns. PBM supports healing in these cases by improving circulation, reducing inflammation, and promoting tissue repair, especially when used alongside standard wound care.
• Peripheral nerve conditions — Damage to the peripheral nervous system can cause burning, tingling, numbness, or shooting pain in the limbs. PBM has been shown to help reduce nerve-related pain and restore some sensory function, particularly in cases of diabetic neuropathy or chemotherapy-induced nerve injury.
Additional studies have looked at its potential to relieve post-herpetic neuralgia (shingles-related nerve pain), improve bladder control, and stabilize blood pressure reflexes, though more data is needed in those areas.
• Musculoskeletal performance and recovery — PBM may influence muscle performance and fatigue depending on dose and wavelength. While further high-quality research is needed, these findings suggest promising uses in sports medicine and physical rehabilitation.
• Cognitive function and neurodegeneration — Though consensus was not reached for all neurological conditions, PBM has been studied for its effects on cognitive performance, memory, and attention. Applications explored in early or experimental studies include brain injury, dementia, chronic migraines, Alzheimer’s disease, and Parkinson’s disease.
I also recently finished a hypothesis paper, which has yet to be published, in which I propose that near-infrared light absorbed by mitochondria triggers local melatonin synthesis, which may activate powerful antioxidant defenses within brain cells. This mitochondrial melatonin system appears distinct from pineal melatonin and operates without circadian rhythms.
According to the model, near-infrared exposure initiates a cascade involving glutathione amplification and SIRT3 activation that offers targeted protection against oxidative stress. I believe this light-triggered mechanism could help defend neurons from age-related degeneration, particularly when combined with adequate intake of glutathione precursors like glycine and N-acetylcysteine (NAC).
• Dermatological and aesthetic uses — PBM has found a place in clinical dermatology, particularly for improving scar appearance and skin rejuvenation. In patients with androgenic alopecia, PBM has also been shown to promote hair regrowth when used at appropriate wavelengths and dosages.
• Oral applications — PBM has been described as generally well tolerated when used for maxillofacial conditions. While the consensus review did not detail specific clinical outcomes, separate research published in The Journal of the American Dental Association reports that PBM may be used as an adjunctive therapy in dental settings to support wound healing, reduce inflammation, and help manage pain.7
As with any biologically active therapy, outcomes depend not just on what condition is being treated, but on how the therapy is delivered. Understanding how to choose the right device — and how to dose it correctly — is essential for translating the science of PBM into safe, practical results.
Practical Guidance for Choosing a PBM Device and Using It Effectively
Using PBM to effectively improve your general wellness depends on both how much light is delivered and how it is delivered. Dose, wavelength, and device quality work together to determine whether PBM produces a meaningful biological response. The aim is to apply enough energy to activate cellular processes without exceeding the range where the effect begins to diminish. Here are some tips to keep in mind:
• Aim for the therapeutic middle range rather than going too low or too high — Research commonly uses doses between 5 and 50 joules per session, with a joule representing the amount of energy delivered in watts per second. This reflects a well-established principle in PBM: insufficient energy produces weak or no biological response, while excessive energy can reduce or inhibit the intended effect.
• Use about 25 joules per session for general whole-body wellness — This level can be reached using a large PBM panel and corresponds to roughly 10 minutes of exposure to the front of the body and 10 minutes to the back. This session length provides enough energy to support cellular signaling and tissue recovery without overwhelming the system.
• Match the device to your health goal, required depth, and daily routine — Consider what you intend to treat, how deep the light needs to reach, and how easily the device fits into your daily routine. Adjustable settings that control wavelength and dosage improve flexibility and help tailor sessions to your needs.
Always choose a clinically validated device from a reputable manufacturer to ensure safety, reliability, and accurate energy delivery. A practitioner trained in PBM can help tailor your dosing schedule based on individual health goals and response patterns.
• Choose a mixed red and near-infrared unit when you want both surface and deep-tissue effects — This device allows you to address both surface-level and deeper tissue issues simultaneously. However, achieving these combined benefits requires spending about 50% more time using the device compared to using a device that emits only near-infrared light.
• Select low-EMF, low-flicker devices to reduce unnecessary stress exposure — Mito Red is one example of a PBM manufacturer that has addressed several common concerns found in many light therapy devices. One of the key features is its extremely low electromagnetic field (EMF) output, measuring under 1 milligauss at a 6-inch distance and dropping to background levels beyond that.
In contrast, some infrared panels emit 5 to 10 gauss or more when used at close range, which may be a consideration for those sensitive to EMFs. They also eliminated light flicker, a subtle but measurable pulsing that tends to occur in infrared light devices and can affect neurological comfort over time. Visit their website to explore the full product line, including portable units, full-body panels for home use, commercial-grade panels, and red-light room systems.
• Consider using sauna therapy — Far infrared saunas, in particular, provide a practical way to deliver therapeutic wavelengths while also supporting detoxification through sweat. Learn more in “Infrared Sauna After Training Speeds Recovery and Supports Athletic Performance.”
• PBM complements natural light exposure — Regular time in natural sunlight remains the best way to receive a full spectrum of beneficial light wavelengths. But for many people, daily exposure is inconsistent or limited by season, lifestyle, or environment. PBM can be a great health investment to fill the gaps when natural light isn’t available, but it’s meant to supplement — not replace — sunlight exposure.
Frequently Asked Questions (FAQs) About Photobiomodulation
Q: What are the benefits of PBM in patients undergoing cancer treatment?
A: PBM is used in cancer care to help manage treatment-related side effects. Clinical research shows it may reduce the severity and duration of oral mucositis, ease pain in the mouth and throat, improve tolerance to radiation-related skin reactions, and support recovery of tissues affected by chemotherapy or radiation.
By helping preserve your ability to eat, speak, and maintain skin and nerve comfort, PBM may also reduce treatment interruptions and improve overall quality of life while you are undergoing cancer therapy.
Q: Why do red and near-infrared light matter more than other wavelengths?
A: Red and near-infrared wavelengths fall within a range that allows light to penetrate tissue without being excessively absorbed by skin pigment, blood, or water. This makes them better suited for interacting with deeper tissues compared to shorter wavelengths.
Q: Should I use blue light as part of PBM therapy?
A: Blue light is included in some technical definitions of photobiomodulation, but artificial blue light exposure can disrupt circadian signaling and sleep regulation. For this reason, focusing on red and near-infrared light aligns better with overall biological health outside tightly controlled medical settings.
Q: Can I use a PBM device at home?
A: Some at-home devices are designed to deliver appropriate wavelengths and doses, but quality varies widely. Look for clinically validated equipment with clear specifications and avoid devices that lack safety certification or accurate output information. Guidance from a knowledgeable practitioner helps reduce misuse.
Q: Does PBM replace spending time outdoors?
A: PBM does not replace natural sunlight. Time outdoors provides a broader spectrum of light and supports circadian health in ways devices cannot fully replicate. PBM works best as a supplement when regular outdoor light exposure is limited by the environment or schedule.
Test Your Knowledge with Today’s Quiz!
Take today’s quiz to see how much you’ve learned from yesterday’s Mercola.com article.
How much does the U.S. spend annually on statins?
Article imported via RSS feed from Mercola.com
RSS Article Source: https://articles.mercola.com/sites/articles/archive/2026/02/14/photobiomodulation-europe-clinical-guide-cancer-care.aspx
